56 yo man with 3 month history of a friable tumor mid lower lip. Non smoker. Works frequently outdoors for years. He has a history of BCC on his back.
O/E: 1 cm nodule lower lip. No palpable regional adenopathy

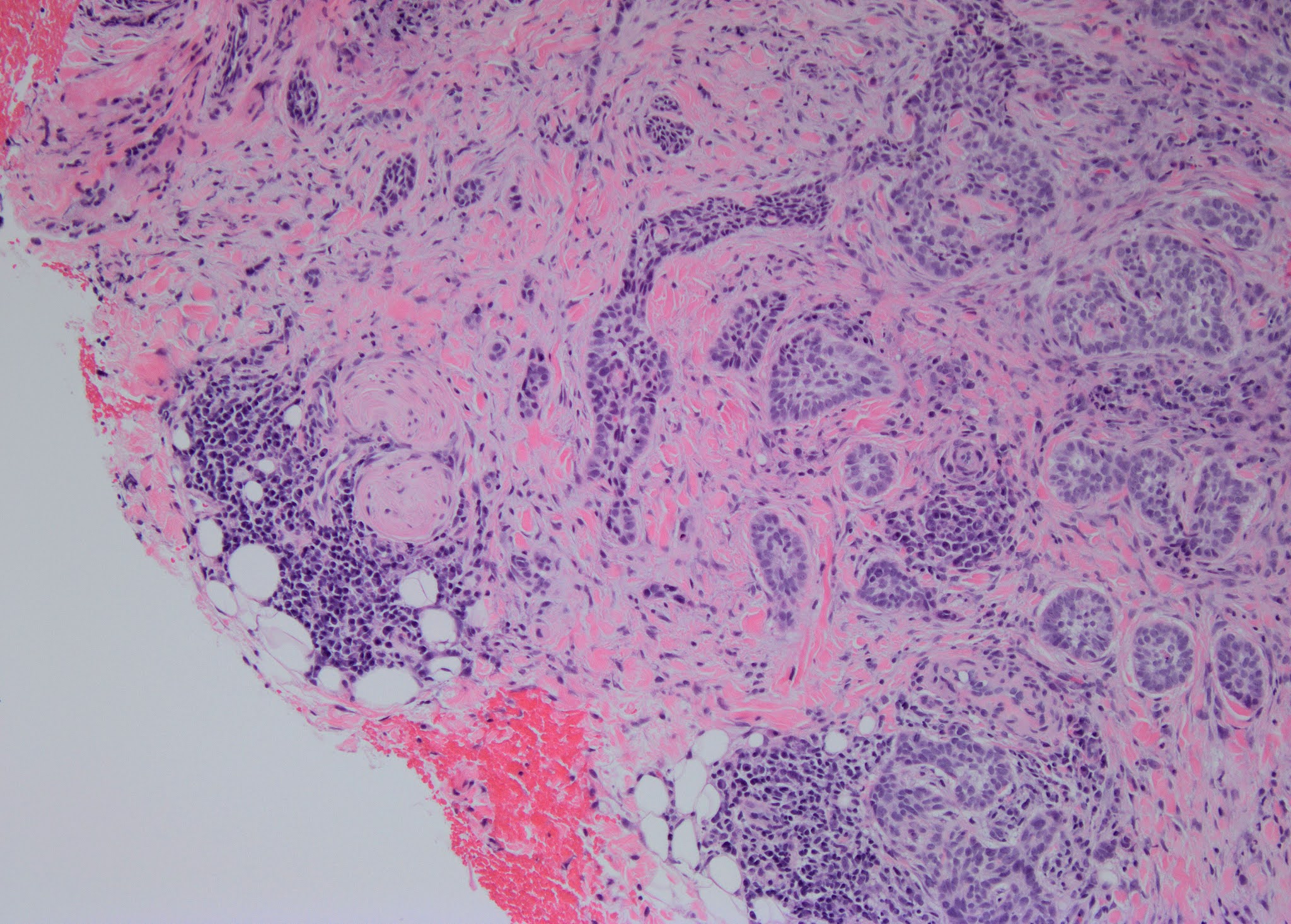
Pathology: Biopsy shows a moderately differentiated SCC with invasion into muscle but no definite perineural invasion or lymphatic invasion on the biopsy. [3 mm punch biopsy may not be representative of the true picture.]
Diagnosis: SCC lower lip, moderately differentiated.
Plan: Refer for micrographic surgery.
Questions:
1. Lip SCC < 2 cm diameter are reported to be at little risk for metastasis. With cases like this should an oncologist be consulted?
2. Is there a role for imaging preoperative imaging?
3. What cosmetic effects of surgery should the patient expect?
References::
1. Squamous Cell Carcinoma of the Lip-A Review of Squamous Cell Carcinogenesis of the Mucosal and Cutaneous Junction. James P Bota. Dermatol Surg. 2017 Apr;43(4):494-506. PMID: 28157733
Abstract: Background: The lip is an anatomic junction for 2 disparate groups of cancer. Cutaneous squamous cell carcinoma (cSCC) is a common malignancy with a favorable prognosis, whereas oral-mucosal squamous cell carcinoma (omSCC) is associated with significantly higher rates of nodal disease and worse outcomes. The squamous cell carcinoma of the lip (lip SCC) is more aggressive than cSCC but less aggressive than omSCC. However, work-up and treatment vary between specialties.
Conclusion: Lip SCC is an overlapping entity that poses many challenges to clinicians. Specialists should be aware of current staging modalities as well as imaging and treatment recommendations to optimize patient outcomes.
Comments from two respected Moh’s surgeons:
1. In part it depends on the depth of invasion. But without perineural invasion, PNI, (defined as SCC cells within the perineural sheath, nerve diameter >0.1 mm if intradermal or involving a sub-cutaneous nerve), this is a low risk lesion. With no palpable adenopathy, imaging is not indicated. Neither is an Oncologist. Mohs surgery or an excision with complete peripheral margin exam is the recommended treatment. If Mohs is done, the remaining clinically obvious tumor can be debulked and sent to path for further review for PNI. Cosmetic insult should be low. If not invading muscle, mucosal advancement flaps can usually close it elegantly. If muscle involved we often do a full thickness "v" wedge repair of the lip. You can close a defect involving 40% of the lip without microstomia and this lesion won't remove even 20%. The lip stretches back to its normal size in a few months. I'm on the NCCN nonmelanoma skin cancer Guidelines of Care committee. We just finished our annual review of the guidelines, which of course cover cSCC an hour ago! So you are getting the most up to date info that can possibly be obtained!
2. This patient looks to have a pretty straightforward case of a SCC on the lip. I don't think you need to refer to oncology or do imaging, given size of tumor, no palpable nodes, no aggressive histology. He needs Mohs and needs it ASAP, as this has grown to 1 cm size in 3 months. Give the Mohs surgeon a heads up that this is growing relatively rapidly. The patient wouldn't want it to increase significantly in size while he's waiting for an appt. This is someone I would have normally given priority to, given the chance for rapid growth. The lower lip is pretty forgiving and if this SCC doesn't grow significantly, the defect could likely be brought together primarily. One can remove up to a third of the lower lip and close primarily without causing microstomia. We know the tumor is into muscle (common on the lip, given thin overlying skin and minimal sc fat), but removing a wedge of muscle will actually help minimize tension on the closure. Tell him stitching will extend into mouth and below the vermillion (to correct the standing cones created with closure). I will send in a separate email a few photos of some prior patients I have closed primarily with this type of defect. Took photo of a scrapbook page, so it may be a little distorted.
I would follow this fellow for the first year after surgery fairly closely (say, q 3 mo) and feel for any palpable nodes.