Abstract: An 84-year-old elderly woman with 3 months history of pruritic skin eruption
History: The patient is an 84-year-old nursing home resident who presents for evaluation of pruritic skin eruption for the past three months. She first noted pruritic lesions on her hands when she was in a hospital for a back surgery. Since then her skin was progressively worsening and the eruption spread to her face, arms, abdomen and legs. She notes she was getting thick scales in the involved areas. She has chronic back pain and has gone through several operations past 3 months. Her other medical history includes congestive heart failure, hypertension, and COPD. Due to pain and her recent skin eruption, she has been taking prednisone, hydromorphone, doxepin, and Ativan. She feels sedated and confused at times. The patient is with her daughter who had significant contact and similar symptoms.
Clinical photos:






Diagnosis: Norwegian scabies
Questions: We'd appreciate your recommendations on this patient's care.
Discussion: Crusted Norwegian scabies is an uncommon hyperkeratotic variant of scabies infestation. Norwegian scabies are known to be as opportunistic pathogens. Our patient has been under significant stress physically and emotionally due to recent back surgeries and her skin eruption has progressed under the eyes of a medical staff. Her medications contributed to the development of Norwegian scabies by suppressing her immune response (prednisone) and blunting her itch perception (Dilaudid, doxepin and Ativan). In a way, this was a perfect storm. Due to severity of involvement, the patient will be treated with oral ivermectin 200 micrograms per kilogram weekly for 3 weeks and permethrin 5% cream weekly for 4 - 5 weeks. Her daughter and all close family members will be also treated with topical medication. The nursing home will be informed. It is estimated that the mite load of patients with Norwegian scabies can be as high as 15 million which accounts for the highly contagious nature of this variant. All of the staff and residents of her nursing home should receive scabies treatment.
References:
1. Towersey L, Cunha MX, Feldman CA, et al. Dermoscopy of Norwegian scabies in a patient with acquired immunodeficiency syndrome. An Bras Dermatol. 2010;85(2):221-223
History: The patient is an 84-year-old nursing home resident who presents for evaluation of pruritic skin eruption for the past three months. She first noted pruritic lesions on her hands when she was in a hospital for a back surgery. Since then her skin was progressively worsening and the eruption spread to her face, arms, abdomen and legs. She notes she was getting thick scales in the involved areas. She has chronic back pain and has gone through several operations past 3 months. Her other medical history includes congestive heart failure, hypertension, and COPD. Due to pain and her recent skin eruption, she has been taking prednisone, hydromorphone, doxepin, and Ativan. She feels sedated and confused at times. The patient is with her daughter who had significant contact and similar symptoms.
Clinical photos:





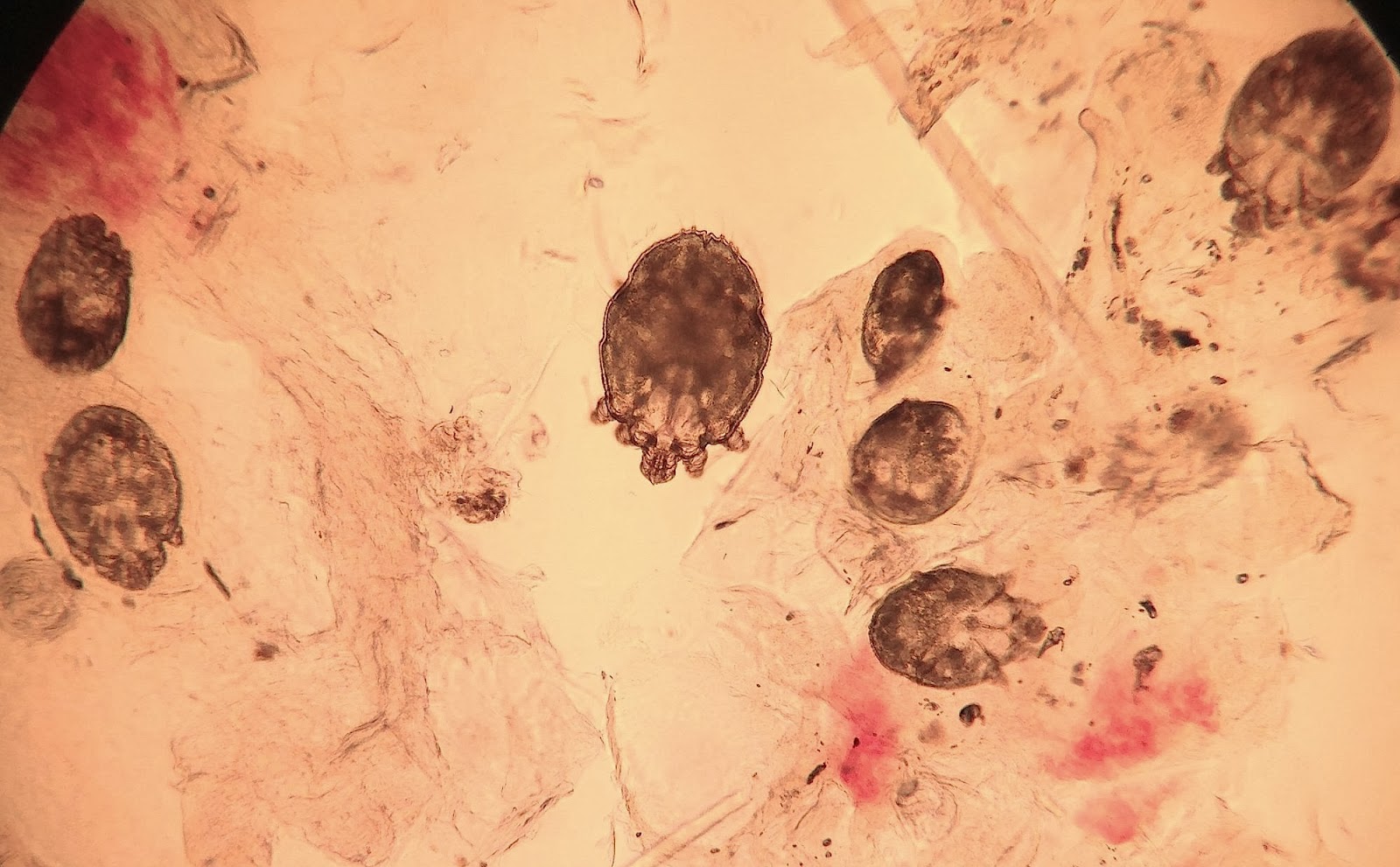
O/E: The skin exam shows a somewhat sleepy, but oriented, elderly woman in a wheelchair with yellow to green thick scaly plaques on the hands, forearms, elbows, face, ears, abdomen and legs. Dermoscopic evaluation shows multiple triangle jet signs with burrows. Scraping prep with mineral oil showed multiple scabies mites. Photo shows a portion of a 10X field on which 11 mites were seen.
Questions: We'd appreciate your recommendations on this patient's care.
Discussion: Crusted Norwegian scabies is an uncommon hyperkeratotic variant of scabies infestation. Norwegian scabies are known to be as opportunistic pathogens. Our patient has been under significant stress physically and emotionally due to recent back surgeries and her skin eruption has progressed under the eyes of a medical staff. Her medications contributed to the development of Norwegian scabies by suppressing her immune response (prednisone) and blunting her itch perception (Dilaudid, doxepin and Ativan). In a way, this was a perfect storm. Due to severity of involvement, the patient will be treated with oral ivermectin 200 micrograms per kilogram weekly for 3 weeks and permethrin 5% cream weekly for 4 - 5 weeks. Her daughter and all close family members will be also treated with topical medication. The nursing home will be informed. It is estimated that the mite load of patients with Norwegian scabies can be as high as 15 million which accounts for the highly contagious nature of this variant. All of the staff and residents of her nursing home should receive scabies treatment.
References:
1. Towersey L, Cunha MX, Feldman CA, et al. Dermoscopy of Norwegian scabies in a patient with acquired immunodeficiency syndrome. An Bras Dermatol. 2010;85(2):221-223
2. Problems in diagnosing
scabies, a global disease in human and animal populations.
Walton SF, Currie BJ. Clin Microbiol Rev. 2007 Apr;20(2):268-79. Excellent review, available open access fulltext.
3. Reflectance confocal microscopy for quantification of Sarcoptes scabiei in Norwegian scabies. Cinotti E, Perrot JL, et. al J Eur Acad Dermatol Venereol. 2013 Feb;27(2):e176-8. PubMed listing.
3. Reflectance confocal microscopy for quantification of Sarcoptes scabiei in Norwegian scabies. Cinotti E, Perrot JL, et. al J Eur Acad Dermatol Venereol. 2013 Feb;27(2):e176-8. PubMed listing.
